|
A child struggling with a bipolar disorder is often highly gifted, but may have difficulty making transitions, and may have co-morbid syndromes that make him or her distractible, inattentive, anxious, or very perfectionistic. He or she may also be sleepy from medications or may be having cognitive difficulties as a result of them. Frequently, children with bipolar disorder have associated learning disabilites and executive function deficits which make it extremely difficult for them to organize and break things down and accomplish complex tasks (we will discuss these executive function deficits in more detail below). All of these co-morbid conditions, medication issues, known and unknown learning disabilities and organizational deficits complicate a student’s acquisition of knowledge and adjustment to academic demands. When one also considers that these children have an illness which causes their ability to focus and energy levels to wax and wane (often according to the season) it’s not hard for parents and educators to realize these children need special accommodations in school. In creating the type of education you want for your son or daughter, you must keep in mind that although all the children we are discussing here have bipolar disorder, each child is an individual with different social, emotional, and academic strengths and weaknesses. Therefore, their educational needs may vary from one season or school year to the next. The JBRF Educational Page is intended to help parents, teachers and the educational team ease the strain for the child struggling with these issues and to ensure a comfort level that allows these students to learn, benefit, and excel in the academic environment. Section 504 Option Versus Eligibility and Classification under the IDEA Once your child has been diagnosed with a bipolar disorder and perhaps a co-morbid condition such as ADHD or OCD and/or learning disabilities of any kind, your child can become eligible for accommodations in the academic environment. He or she is protected by two federal laws: Section 504 of the Rehabilitation Act of 1973; and the more powerful statute enacted in 1975 and reauthorized in 1997 known as the Individuals with Disabilities Education Act (IDEA). Section 504 mandates that individuals with impairments that substantially limit a major life activity, such as learning, are entitled to academic adjustments and auxiliary aids and services, so that courses, examinations, and services will be accessible to them. Parents often ask why they should certify their child under the IDEA instead of under Section 504. A Section 504 is intended primarily for use in the mainstream classroom. If a child needs minor accommodations such as a bathroom pass because he or she has frequent urination as a result of a drug such as lithium, or needs seating close to the teacher so that he or she can pay better attention, then accommodations under Section 504 may be adequate. However, bipolar disorder is by nature an episodic illness which may become acute at times. A student with this illness typically needs more services outside the classroom and may need accommodations such as time spent in a resource room, an aide, or a later start to the school day (these accommodations will be explained in the pages below). These more flexible, all-encompassing accommodations are rarely available unless the student has an Individual Education Plan provided by an IDEA classification. (The IDEA provides federal funds to elementary and secondary schools for public education, whereas no such funding supports a Section 504.) In other words, accommodations under a Section 504 may work as an emergency measure while the IEP process is being conducted (to help ease the stress on the child) but they are probably not adequate for the majority of children with bipolar disorder throughout the span of their time spent in school. Under IDEA, schools are responsible for identifying and evaluating students with disabilities who may need special education and services. This federal law also requires schools to continue providing services for the student as long as they are needed through their K-12 schooling and up to age 22. The services are provided through a plan or blueprint called an Individualized Education Program—the IEP. Before the IEP can take place, however, the student must be tested and found eligible for services. For your child to qualify for special education under IDEA, it is not enough that he has one of these disabilities. There must also be evidence that your child's disability adversely affects his educational performance. There are 13 categories under IDEA which entitle a child to services and accommodations throughout the school day. The two that most often apply to a child with a bipolar disorder are “other health impaired” (OHI), or “seriously emotionally disturbed” (SED). The SED classification may be referred to in some states as “emotionally disordered” (ED), behaviorally disturbed (BD), or some variant of these. The phrase “severely emotionally disturbed” may sound exceedingly ominous to parents, but in some states an ED label may make it easier to access better services such as out of district placements or a therapeutic day school or residential school if this becomes necessary. If parents do accept this label, they must be certain that the ED classification (and the IEP team) does not place the child in an inappropriate placement with students who have more delinquent behaviors. Since every state has different laws and ways of classifying students, it may be best to speak with an educational consultant or educational attorney before setting out on this journey. To locate a trained advocate or attorney see the Resource section provided here. Initiating the IEP Process A child cannot receive services until a full evaluation is completed and the child has qualified as disabled under the IDEA. A parent should request an evaluation in writing after having first talked with the special education director and guidance counsellor to find out how their system initiates the process. In many states, the parents are asked to sign a consent form which makes their child a “focus of concern.” Once the process begins the child will be observed in the classroom, and a number of standardized tests that assess IQ, academic strengths and weaknesses, and language and communication abilities will be administered. Various psychological assessment tests may be administered as well. Additionally, an observation by a qualified person (such as the school psychologist) must be made as part of the assessment to qualify and place a student in an ED program. All the testing will be done by the school system at no expense to the parents. However, parents may bring their own independent assessments to the meeting. Doing so allows a parent to handpick an experienced tester who will do more in-depth testing and supply a very specific report. Since the IEP is the critical document from which all services and progress benchmarks flow, the quality and comprehensiveness of the baseline assessments cannot be underestimated. The professional most qualified to provide this kind of focused assessment is a neuropsychologist—for all the reasons we are about to discuss. The Neuropsychological Testing of a Child with Bipolar Disorder
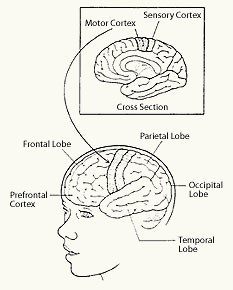
Not only do the symptoms of a mood disorder impact a child’s ability to learn, but evidence is emerging that learning disabilities, attentional problems, and deficits in the area known as executive functions are a significantly associated feature of early-onset bipolar disorder. A learning disability is assumed to be present when a child has a discrepancy between his or her ability and his or her achievement. This is typically documented when a student has a normal or high IQ, but is still two years behind his or classmates in academic learning. U.S. Public Law states that learning-disabled individuals are: “Those who have a disorder in one or more of the basic psychological processes involved in understanding or in using language, spoken or written, which disorder may manifest itself in imperfect ability to listen, think, speak, read, write, spell, or do mathematical calculations.” These are broad and rather non-inclusive definitions of learning disabilities which address mostly verbal disabilities and which fail to take into account the non-language domains and area of executive functions. A specific learning disability is a breakdown in one particular task area, whereas executive function deficits cut across many domains and impact all arenas of life—both academic and non-academic. Executive function deficits affect the student’s ability to organize, strategize, and plan, among other things. It is highly likely that deficits in the area of executive functions will not be apparent until schoolwork gets more complicated, requires more independent work, and more planning and strategizing. Therefore, unless a child is tested and identified as experiencing these deficits, the snowballing effect of problems in this area may not become apparent until middle school or early high school. If the child shuts down and refuses to do school work at this point, parents and therapists will look to medication failure and the thriving of hormones before thinking that it may be “silent” executive function deficits. Therefore, children with bipolar disorder should be tested with a comprehensive battery of intelligence, academic, neuropsychological, and psychological tests. These tests identify area of strength and weakness and do much to explain present difficulties and warn of future difficulties as the academic work-load becomes more demanding and intense in the higher grades. The findings of these tests will guide remediation efforts, and are critical when developing the Individual Education Plan—the IEP. Who Should Test and How Do You Find The Tester? Children with bipolar disorder should be tested by a child neuropsychologist. This is a professional who has specific training and supervised experience in the assessment and treatment of patients with brain disorders, and disorders of the central nervous system. A neuropsychologist typically has a doctorate in psychology and two years of postdoctoral training within a neurological or neurosurgical setting (one year in a general setting; one in a children’s unit). These professionals are licensed by the state. To find a neuropsychologist, speak with your child psychiatrist, pediatrician, or pediatric neurologist. Other health professionals, such as occupational therapists, physiotherapists, speech pathologists and special educators may also make referrals. Remember, you are looking for someone who does more than psychoeducational testing. A comprehensive battery of tests can easily require eight hours of direct consultation, as well as additional hours for reviewing records, data analysis, and the preparation of a written report. The cost for such an assessment will run in the range of $2,400-$3,000. Some insurance companies may reimburse a portion of the fees, but many do not. It’s a good idea to call your insurance company for preauthorization. The school’s assessment will not be a complete neuropsychological evaluation since most school psychologists are not licensed to administer and interpret the neuropsychological battery of tests. Some schools may accept the test results that you bring them and be heartened that a seasoned professional has pinpointed areas of difficulty. However, the IDEA does not require them to accept your professional’s findings. In the event the team does not consider the findings in an independent or outside assessment, you have the right to present your findings in a due process hearing. In such a case you will want to consult with a qualified education advocate or attorney. (See Mediation and Due Process below.) The Battery of Tests: A suggested battery of tests (including the battery that examines the domain of executive functions and that should be given to all children and adolescents with bipolar disorder) is listed and discussed in depth in The Bipolar Child, Revised Edition. For the purposes of this article, we will focus only on the executive function deficits that so many children with bipolar disorder are now suspected of having. What Are Executive Functions? The pre-frontal cortex and the frontal lobes which are (just in front of the motor strip), are the areas of the brain that coordinate speech, reasoning, problem solving, strategizing, working memory, attention, self-control, intention, motor sequencing, and other processes central to higher functioning. When all is well, an individual can plan, strategize, break a plan down into smaller tasks in order to aim for a goal, assess if the strategy is working or not and be flexible enough to change it (“shift set”), bring working memory to bear, and sustain attention and see the project through to the finish.
Research is showing that children with attention-deficit disorder with hyperactivity, as well as those with Tourette’s syndrome, have deficits in the frontal lobes. It is now suspected that many children with bipolar disorder also have problems in the frontal lobes. When the prefrontal systems don’t work correctly, there is a major impact on the ability to pay attention, inhibit impulses, devise plans, carry them through, and alter them if needed. The child with glitches in this area will appear distractible, impulsive and restless, and disorganized (things will be lost or forgotten; rooms will be a mess). The problem or problems in the domain of executive functioning, governed by the frontal lobes may account for the co-morbidity between ADHD and bipolar disorder, Tourette’s syndrome and Oppositional Defiant Disorder. Working Memory Working memory is often confusing to people who understand short-term memory and long-term memory. An excellent definition of working memory is provided by Dr. Leslie E. Packer: “When you hold new information in mind while you retrieve past information to apply to it, you are using your working memory. If I ask you a question, you keep the question in mind as you mentally search through your ‘memory files or folders’ to pull out the information you are looking for. But what if memory’s ‘filing system’ is a disorganized mess? You’d know that the information was ‘in there’ but it would take you longer to find it and you may not always find it in time.” Working memory, then, involves the ability to hold data in short-term memory while manipulating it toward problem solving or sequencing it in a logical order. Research studies using functional magnetic resonance imaging (fMRI) have examined working memory and found that as memory load grows heavier, activity increases in the front area of the brain. A key part of the prefrontal cortex and certain other brain areas stay active, impressing researchers that these areas are involved in the active maintenance of information in working memory. Bipolar children also seem to have problems with working memory. This is not surprising since they seem to have some problem in the prefrontal cortex of the brain. Motor Skills Executive functions also affect motor skills as the motor strip begins the frontal lobes. (If you think of the placement of a headband on the hair, imagine the motor strip there, and everything in front of it the frontal cortex. The prefrontal cortex is the layer of tissue just behind the forehead). Almost all tasks—by definition—involve not only analysis, planning, monitoring, and adjustment of strategy, but also images and ideas which must be translated into sequenced motor acts. It is not uncommon for these children to have difficulties with fine motor skills (handwriting) and motor outflow (initiating action in space). This is the child who may appear lazy, unmotivated, and hopelessly disorganized. As one very bright boy put it: “Remote controls were made for people like me.” Parents can read about the problems that executive function deficits can cause for a student at school at http://www.schoolbehavior.com/conditions_edf.htm. There are some excellent tips for educators and parents on how to better organize the child or adolescent. We particularly liked the picture of the backpack and its being labelled “Another black hole in space where papers and books disappear never to be seen again.” How to Prepare for the IEP Meeting The maximum amount of time allowed to pass between the parents’ request and/or agreement to conduct the evaluation to the IEP development differs from state to state, but most regulations cite a time line somewhere between fifty and 120 days. (Note: In some states the meeting at which the IEP is written is called by the somewhat misleading phrase Admission, Review Dismissal meeting–the ARD meeting.) Whatever it’s called in your state, you will have a lot to prepare so that the meeting is productive and so that the school personnel understand the necessity of the accommodations. Being prepared will also ensure that the IEP is well written. Parents must be prepared to educate the school team, develop a resource binder, rehearse the meeting beforehand, and decide who will be at the meeting with them (the child psychiatrist, an advocate, an educational lawyer?). Any written materials about early-onset bipolar disorder that you want the special education team at school to review (perhaps this article, and the FAQ from this site http://www.jbrf.org -- click on “About Juvenile Bipolar Disorder”) should be sent about two weeks before the scheduled meeting so that the IEP team will have time to digest the materials and better understand how to write the IEP. Few could skim and grasp the implications of this illness and construct an IEP in the hour or two allotted to the process without prior knowledge about the student’s challenges and illness. Preparing the Binder The three-ring binder should carry a picture of your child on the front, his or her name and grade on the spine, and be divided into sections inside. These should include:
Educating the Team About Accommodations That Will Benefit Your Child Since a parent usually understands the illness and the side effects of the medications better than anyone, he or she should be ready to spell out a list of symptoms and medication side effects and proposed modifications in the academic schedule to accommodate the child’s difficulties and to make the school day more productive and comfortable for the student. Hopefully, by the time the education team sits down to write the IEP, the parents can provide the independent neuropsychological assessment which can pinpoint any specific learning disabilities, learning styles, and possible weaknesses in the domains of executive functions. (This neuropsychologist’s report should make recommendations for the academic arena and these recommendations should be addressed in the IEP also.) We thought it would be helpful to divide the modifications into categories where parents and educators could see at a glance which symptoms the student has and which accommodations will have to be incorporated into the IEP. Four categories the IEP team should consider when developing an appropriate IEP for a student with a mood disorder are:
(Click here to view all the symptoms and accommodations) The Individualized Education Plan, constructed by the school team, is a written statement of the goals, objectives, and services that will be provided to assist a child with exceptional educational needs. A well-written IEP will incorporate long term goals and very specific measurable objectives accompanied by a timetable in which those objectives will be met. Federal law mandates that an IEP include seven required parts:
The IEP goals should be written for all academic areas of need (math, reading, writing, etc) and for any school-related areas of need (such as attendance, school behavior, self-help, social, emotional, etc.) The language should be very specific. In addition to the written goals, the document should answer the following questions:
To view a model of an IEP written specifically for a student with bipolar disorder, go to The Bipolar Child website: “Model IEP.” The goals of the IEP should be monitored and reviewed every nine weeks to determine if progress is being made. Parents may request more frequent feedback. Additionally, parents may request an IEP meeting at any time to review progress and to request needed changes. Though the school is required by law to conduct a triennial review (every three years) where the student will be retested, this is generally too long to wait to determine if the student’s academic weaknesses are being remediated. We advise parents to have an annual, independent evaluation in early spring so that a meeting can be called and the results of any evaluations can be shared with the IEP team. This will ensure that the appropriate program, goals, and objectives are in place for the next school year. Some states and school districts require and regularly provide annual reviews. Annual reviews do not require a complete neuropsychological evaluation. Instead, they focus on troublesome areas that are being remediated in school or with private tutors. Do not assume your child will tell you (or be able to identify) that he or she is having a problem or that the work is too difficult. Instead, they become Masters of Defense and develop the attitude “Who gives?” Also, understand what “grade level” means. If a dyslexic student has a verbal IQ of 138 and her reading is “at grade level,” assume that this is a near-tragic scenario. Any child doing work three standard deviations below his or her cognitive ability (no matter what the learning disability) is a child in trouble. Some schools may not recognize this or wish to point it out to parents as they fear a due process hearing. What If the School is Non-Compliant with the IEP? An IEP may be beautifully written with the best of intentions but a parent may begin to notice that the mandated services are not being provided, or are being provided inconsistently. This may occur when mainstream teachers ignore the modifications and/or accommodations set down in the student’s IEP. The parent has not only to question this, but must document it as well. The parent’s first course of action is to remind the school in writing that they are required to follow the IEP. The more documentation that a parent has, the better the case that he or she will be able to advocate for the child if corrections are not made and the situation heads to mediation or due process. (Hearing officers do not like to see that schools are out of compliance with an IEP so a parent needs to document carefully.) Any omission of an accommodation or a service should be noted in a log by the parent, and a letter detailing this omission should be sent to the special education teacher with copies to the school administrator and program manager at the district level. If the matter is handled over the telephone, a letter should be written as a follow-up to confirm the content of the discussion that says: “This is to follow up in writing what we discussed on the telephone today…” If matters do not improve with dialogue and follow-up documentation, a parent should contact his or her state’s Protection and Advocacy group. This is a nationwide network that, among other things, devotes considerable resources to ensuring full access to inclusive educational programs. A phone call or letter from the Protection and Advocacy group requesting accommodations or that accommodations already in place be complied with, or the presence of one of the P&A personnel at an IEP meeting almost always ensures things happening. To find the Protection and Advocacy group in your state, call the National Association of Protection and Advocacy Inc. at 203-408-9514; or visit their web site at http://www.protectionandadvocacy.com and click on “P & A’s/CAPS. If matters still do not get resolved, the IDEA includes rules of procedure for resolving such complaints. These rules include mediation, due process hearings, and appeals to the state or federal courts. (See the section on Mediation and Due Process Hearings below.) Functional Behavioral Assessments and Behavior Intervention Plans
While many children with bipolar disorder don’t act out in school (but save their pent up frustration and upset for home and mother), some do. The school may try to discipline, suspend, or expel the student due to unruly or oppositional behaviors without understanding that many of the behaviors are a result of the student’s condition. If you or the child psychiatrist believe that these behaviors are sequellae of bipolar symptoms, you should request that the school conduct a Functional Behavioral Analysis (an FBA). Based on the findings of the FBA, the school must write a Behavior Intervention Plan (BIP) into the IEP. This is now mandated by law. The FBA/BIP Process The FBA (Functional Behavioral Analysis) is a formal assessment which can identify problem behaviors a student is exhibiting, where they are having them, when they are having them, and with whom they are having them. The data is analyzed and a Behavioral Intervention Plan is developed which provides goals to replace problem behaviors with positive behaviors. Only trained professionals such as psychologists or special education teachers with specialized training are qualified to conduct a Functional Behavioral Analysis. We cannot stress strongly enough that parents need to investigate the level of experience of the people assigned to conduct the FBA. If it becomes obvious that experienced professionals are not available, then the parents are going to have to insist that the school district bring in such professionals from the outside. Otherwise school districts will continue developing BIPs which are inherently flawed and subject to failure. The data from the FBA is used by the BIP team (school psychologist, teachers, support teachers and any other professionals who work with the child) to develop an appropriate intervention plan that will:
The school will implement the plan and, over time, evaluate the outcomes as outlined in the plan. It is important when observing a child with bipolar disorder to differentiate between behaviors that can be modified, and symptoms of the illness. For example a child may be refusing to work because he is overwhelmed by the stimulation in the room, does not understand the assignment, and/or feels lethargic from the meds and/or the illness (or a combination of these factors). Therefore, he is simply not able to perform to the teacher’s expectations at that time, as opposed to being defiant to earn the respect of his peers, or some other outcome (known as a function) of the behavior. It may be necessary for the team to receive training in childhood bipolar disorder before the team is able to create an effective and appropriate Behavioral Intervention Plan--one intended to identify the antecedents of the problem behaviors and modify them with positive behaviors. The Behavior Intervention Plan should:
Some examples of these interventions are:
For more information about FBAs and BIPs, contact the Center for Effective Collaboration and Practice. This is a national organization that helps students with emotional and behavioral problems in school. Go to http://cecp.air.org/fba/default.htm Two other helpful sites are: http://www.ed.gov/databases/ERIC_Digests/ed429420.html Where Can The Student’s Needs Best be Accommodated? Because federal guidelines call for placing any child with a disability in the least restrictive environment, most public schools begin providing services in the regular classroom. If the child continues to struggle or does not make progress in the general education classroom, the team may decide (with the parents’ agreement) to place the child in a self-contained classroom within the public school setting. Here the class size will be reduced and there will be more accountability to the individual student. There are typically one or two special education teachers and a trained aide or two working with the student in the self-contained classroom. Depending on the student and the special ed program, the child may be “mainstreamed” into regular education classes for some academic subjects and for elective periods such as music, art, gym, computer, etc. The time may come, however, when it becomes clear that a small, therapeutic program in a private or public school would be a more appropriate placement for the student. When a student’s illness negatively impacts his or her learning and no progress is being made academically, socially and/or emotionally, the parents and school team should begin to discuss a therapeutic day school. This is a separate school, usually with a small number of students, a small class size (six to eight children), in a classroom with a trained special education teacher and a trained aide. The child receives academic instruction along with group therapy, individual therapy, social skills classes, and art and music therapies. Some schools will make recommendations of therapeutic day schools, but some will tell parents only about programs that are inexpensive for the school district and which may serve more as a warehousing situation than an appropriate place for education. Nor will all communities have any kind of therapeutic day school—good or bad. In these situations, parents will want to contact an educational consultant (and may have to secure the services of an educational attorney). The Independent Educational Consultant Association has a list of reputable consultants in all areas of the country. Go to http://www.iecaonline.com or call 703-591-4860 to obtain names and phone numbers. Educational consultants are trained experts who possess comprehensive knowledge of placement options. Many consultants specialize in crisis-intervention and have extensive experience advising families with children who have emotional and behavioral difficulties. This expertise is used to advise you on the most suitable placement for your child. Parents can also contact their Department of Education’s Special Education Division. Most states list their approved therapeutic day schools so you can at least get started. Go to: http://www.ed.gov/Programs/bastmp/SDSE.htm Therapeutic Boarding Schools and Residential Treatment Centers Therapeutic boarding schools are generally middle schools, and high schools that have comprehensive therapies for the students and a program to help them with self-esteem and problem behaviors. Some of them are “character building” schools, and all have individual philosophies. At this time most of the therapeutic boarding schools do not have a medical plan for bipolar disorder, and do not provide psychiatrists on staff. If you want your child to attend a therapeutic boarding school he or she needs to be stable enough to attend school with therapy support, while maintaining a relationship with an outside psychiatrist. Additionally, some schools do not wish to administer psychotropic meds. Residential Treatment Centers Sometimes the school that best meets the child’s needs just doesn’t exist anywhere near the child’s home, or the child may become too unstable to stay at home and attend school. It may become painfully obvious that a change in environment with a twenty-four-hour peer group and nonparental authority figures may help the child blossom and mature in a safe environment. Maybe they are a danger to themselves or to others and they need to be in a setting that can monitor their illness, as well as provide them with tools to understand and deal with their illness. Residential Treatment Centers (RTCs) are medical facilities. They have psychiatrists and nurses on staff. They administer medications, make medication adjustments, and provide therapy and schooling. They are required to follow a student’s IEP. Residential schools can cost anywhere from $56,000 to over $125,00 per year. A school district may pay part or most of the fee of such a placement, but typically only after a due process hearing. Parents should definitely seek the help of a professional consultant and the child psychiatrist should be involved with the search process. Websites that are particularly helpful are: Family Light --also known as Bridge to Understanding http://www.bridgetounderstanding.com; Peterson’s http://www.petersons.com (check under special education); and Ron Woodbury’s Struggling Teens http://www.strugglingteens.com; The American Association of Children’s Residential Centers http://www.aacrc-dc.org. Some parents will need to go to mediation or due process to achieve the proper educational accommodations or educational setting for their children; and this is where the relationship between school and parents enters the legal arena and the relationship becomes adversarial. It is not recommended that parents go through this process alone, so parents will need to procure the services of an experienced educational attorney. The decision to pursue due process is a very serious one as the costs--financial and emotional--to the parents can be enormous. To explore the pros and cons in full, first read the education chapter of The Bipolar Child, Revised Edition, especially pages 307-310; and be prepared to spend multiple hours at http://www.wrightslaw.com --the gold standard of the rights of special needs students. To locate an educational attorney, go to http://www.abanet.org and http://www.copaa.net
Homebound instruction is considered a “general education” placement, but it is considered the most restrictive placement because it removes the student from the mainstream and peers. However, it is frequently used for a student who is too symptomatic, or too emotionally fragile to attend school in the school building. It is considered a temporary placement until the student is able to return to school or until a more appropriate placement can be procured. Parents need to know that a doctor’s “order” must accompany the request for home instruction. An IEP meeting will determine how often the tutors for each subject will come to the house to provide instruction and lessons for the student. Some school districts require a doctor’s therapy or treatment plan to accompany any application for homebound instruction. If an appropriate learning situation is not available in your geographic region, and if the stresses of school—any kind of school—are making it difficult for the child to function, or to recover from an episode or hospitalization, some parents may want to consider the option of homeschooling. Homeschooling was viewed, not too long ago, as very counterculture, or something that people did solely because of religious beliefs. As outcomes of homeschooling were measured, however, and the homeschooled children often tested two years ahead of their in-schooled peers, homeschooling has become more generally accepted. All 50 states allow for it as long as the parent completes the necessary paperwork with the state’s department of education. To locate your state’s DOE, go to http://ucasdweb.iu5.org/Learner%20Links/stdpted Thanks to advances in technology, homeschooling can be done richly and effectively on computers with CD-Rom curricula or even over the Internet. This mode of learning may be particularly beneficial for a bipolar child because it focuses learning and helps students with attentional problems. One such curriculum, Switched-On Schoolhouse, is an advanced multimedia-based learning environment that incorporates video clips, sound files, animations, computer games, drills and tests. With earphones, a parent can homeschool several children. The student works at his or her own pace and if a hospitalization should interrupt learning, the student doesn’t miss the work but just picks up where he or she left off. Switched-On Schoolhouse has curricula for grades 3-12, but it is a Christian curriculum with some religious content woven sporadically throughout the text. If this is an issue, a similar secular program is available from Pathway Publishers and is called “Odyssey Ware” (see homeschooling web sites below). The availability of special education services for homeschooled children varies from state-to-state. Some states may consider a homeschooled student to be enrolled part-time in the local district; in this case, the district would continue to provide full or partial services under an IEP. Other states classify homeschooling as private schooling, so the student is not entitled to an IEP. (However, the student may qualify for a services plan. See http://www.ideapractices.org/law/briefs/brief10.php for a description of the law when parents place their child in a private school.) You will need to research the practices and options in your state and local district. Start with your state's Department of Education. The following link may help you determine the current status of special ed services for homeschoolers in different states: http://www.hslda.org/search.asp. To further explore the prospect of homeschooling, or to take a look at programs that may help a child catch up when work is missed, take a look at the following web sites: http://www.home-school.com --Official web site of Practical Homeschooling Magazine, Listing of homeschooling organizations in your area, Home Life Catalogue, Discussion forums. http://www.HSLDA.org -- The Home School Legal Defense Association http://www.network54.com/Forum/180575-- Interesting discussion forums for parents who are or are thinking about homeschooling. http://www.aop.com -- Switched-On Schoolhouse ‘s CD-Rom Curricula and other Alpha Omega products http://www.pathwaypublishers.com (Odyssey Ware CD-ROM curricula, the secular version of Switched-On Schoolhouse) ttp://www.welcometoclass.com -- On-line accredited schooling from Alpha Omega Publishers (interactive schooling with teachers, counsellors and support staff) http://www.saxonpublishers.com
To read the story of two parents and the school they founded to serve the needs of children with bipolar disorder and their families using a CD-Rom curriculum that makes such a school economically feasible, go to http://bipolarchild.com/newsletters/0110.html.
FINAL WORDS Any questions you have regarding your child’s education can be asked of and discussed with the JBRF educational team and other parents and educators who visit this site simply by clicking on the Educational Forum. We look forward to your visit and to getting to know you. All best, Mary Jane Hatton and Sandi Norelli, Co-Directors, the JBRF Educational Team This article was written by Janice Papolos (co-author
of The Bipolar Child, Revised Edition), Mary Jane Hatton, and Sandi
Norelli, (co-directors of the JBRF Educational Team), Christine
E. Garcia, M.Ed., and Anne Marie Smith, M.Ed. http://www.jbrf.org
|
|
Go
To JBRF's Online Educational Forum Educational Forums Home
Page |
|||||||||||||||||||||||||||||||||||




Top | Home | About JBRF | About Juvenile Bipolar Disorder | Research Studies
Professional ListServs | JBRF Library | In The News | Make A Donation
Our Disclaimer | Privacy Policy | Contact
Web
site designed by flyte new media
email
Web Developer