|
Why Define a New Phenotype?
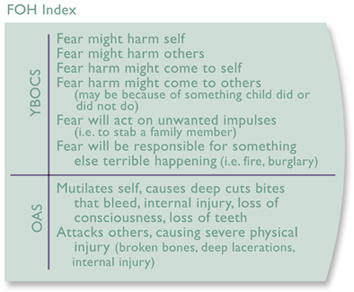
It has become apparent to many psychiatric researchers that the manner in which most mental disorders have been defined since the early 1980s may not be so helpful in our quest to explore and understand their biological roots. Current diagnostic definitions, conceived of under the assumption that there are strict boundaries between disorders, attempt to pare down an illness to include only those symptoms thought to be most directly related to it. This approach excludes a symptom from a diagnostic definition if it could be considered more directly relevant to an alternate illness. Hence, in this scenario, the definition of bipolar disorder is primarily shaped by symptoms of mania and depression. The anxiety, aggression, obsessive-compulsive behaviors and other symptoms which so often accompany a bipolar condition are cleaved off and assigned to different diagnostic groupings. The approach is called categorical because it attempts to separate symptoms into discreet categories. Psychiatry has been using these classifications for the past 30 years and they have been very helpful in the standardization of diagnoses. However, the process that created these diagnostic definitions was not derived from scientific evidence. Rather it was diagnosis-by-consensus based upon the best clinical knowledge available at the time. Regardless of how enduring or universally accepted these diagnostic constructs have become, they were always meant to be changed based on new research findings. Necessarily relying upon categorical classifications to gather study subjects, genetic and neuroimaging studies have had limited success in finding the causes that underlie complex mental disorders such as bipolar disorder. Although research subjects may share the same diagnoses, it seems that categorically constructed diagnoses may not be a useful guide to identify those individuals who share similar genetic or neurophysiological characteristics. This may account for the lack of meaningful results that has subsequently stalled efforts to find more targeted treatments. In response, investigators are beginning to conceptualize mental disorders in a new way. This new approach rejects the previous categorization of exclusive symptoms. Instead, it accepts the inevitable overlap of symptoms between disorders. Further, it quantifies the relevance of those symptoms based on degrees of severity and heritability. Under this construct, mental illness is regarded as a matrix of behavioral and/or functional dimensions each made up of a particular cluster of symptoms. This conceptualization is called a dimensional approach. Drs. Kendell and Jablensky have written an article that explains dimensional analysis more fully: Distinguishing Between the Validity and Utility of Psychiatric Diagnoses. American Journal of Psychiatry 2003; 160:4-12. http://ajp.psychiatryonline.org/cgi/reprint/160/1/4 While multiple dimensions of clustered symptoms may seem to cast a wide and loose diagnostic net, the combined orchestration of symptoms actually provides much more specific criteria than traditional diagnostic definitions. Further, the sets of traits that they identify are more developmentally predictable than the stripped down symptom lists of categorical definitions. The clearer, more refined description afforded by the dimensional analysis increases the chances of gathering a pool of individuals who are genetically similar. By even further dissecting that profile into subgroups based on the heritability of certain traits, the chances for identifying a homogeneous study population are greatly enhanced. In genomics, the importance of analyzing symptom dimensions as a strategy for genotyping is becoming more evident. For a genome-wide linkage scan in a large sample of bipolar adults, Cheng et al. (2006) used both standard diagnostic models and the comorbid symptoms of psychosis, suicidal behavior and panic disorder to identify phenotypic subtypes. Over half the regions implicated by the strongest linkage signals (genome-wide significance) were identified by the phenotypic subtypes. Cheng and colleagues concluded that a dissection of the disease phenotype can enrich the harvest of linkage signals and expedite the search for susceptibility genes.1 In neuroimaging studies of children with obsessive-compulsive disorder (OCD), researchers broke down the subject pool by distinguishable traits such as washing and checking. By doing so, they were able to visualize specific neural circuits that identified those discrete features. This clear association with a biological correlate would have been obscured if they had used the diagnostic nomenclature of DSM-IV.2 Not only may a dimensional analysis provide a more accurate route for defining homogenous behavioral subtypes, but the landscape of symptom-clusters that it reveals may more readily suggest particular biological correlates. The identification of that correlate is advantageous for two reasons. First, it provides a context and focus of inquiry that may be new and revealing and which could suggest novel therapeutic approaches. Second, it could lead to the identification of quantifiable, distinguishing biological markers that could guide differential diagnosis. There is really no codified road map to help determine the dimensional matrix of an illness. Indeed, the quantification of unwieldy behavioral dimensions has deterred this line of thinking in the past. However, rigorous statistical methods are now available that can sort and quantify data; clustering together those symptoms that significantly associate with one another. It is these clustered symptoms, technically referred to as factors, that suggest a dimension of behavior or functionality. Each factor is named according to what its particular mix of symptoms suggests. Some examples of factor names would be sensory sensitivity, territorial aggression or sleep/arousal. Looking at the factors that are found to be the most significant can provide an alternative, and perhaps even more clinically relevant, view of the characteristics that are most important in a disorder. This may lead to novel insights and new research that prompt further dimensional refinements of the behavioral subtype. This is the process which Dr. Demitri Papolos and an interdisciplinary group of researchers from around the country have pursued to arrive at their Fear of Harm phenotype of juvenile-onset bipolar disorder. The Fear Of Harm Phenotype Summary For more than a decade, Dr. Papolos and his colleagues have sought to gain a clearer understanding of juvenile bipolar disorder. Given the terrible lack of consensus in the psychiatric community regarding the diagnosis of this condition, these researchers elected to use a dimensional approach to explore the conundrum and hopefully to provide a better characterization of the illness. Indeed their work has allowed them to conclude that, in addition to depression and mania, a variety of other symptoms are part and parcel of the illness and that some of those symptoms may actually eclipse mania and depression for diagnostic and genetic relevance. While their studies demonstrate that a very large majority of children who had been diagnosed in the community, or were at risk for juvenile bipolar disorder, are indeed significantly impaired, investigators were able to define a subgroup of children who are at greatest risk for the most severe form of this manic/depressive syndrome. They call this subgroup the Fear of Harm (FOH) phenotype. In addition to the high risk of self injury, injury to others and suicide threat that are important characteristics of this phenotype, children in this group also experience an early age of onset, severe manic and depressive symptoms, early and frequent psychiatric hospitalizations, significant social impairment and school problems. Fortunately, the same questionnaires that were instrumental in identifying this high risk group can easily be used within a community setting to screen for children who fall into this category. Six factors derived from the symptom list of the CBQ (Child Bipolar Questionnaire; a screening tool which will be described below), can identify this phenotype with 96% accuracy. As we all know, early detection greatly improves a childs outcome by setting into motion early intervention. Beyond the clinical significance of the phenotype, it also has great research potential. The strong heritability of its defining dimension makes it an excellent candidate for a genetic inquiry. The ability of the CBQ to accurately, easily and rapidly identify FOH subjects increases the likelihood that a large, homogenous pool of DNA can be gathered, thereby increasing the chances for a reproducible genetic study. Whats more, the dimensions that have been identified suggest a neurobiological model of the illness. That model includes a physiological marker and has led to the hypothesis that the orexigenic neuropeptide circuit, a circuit that modulates arousal, sleep onset and offset, REM propensity, appetite, fear sensitization, reward, territorial aggression and body temperature rhythms, may be the underlying biological correlate of the phenotype. This potentially important phenotype, defined by the Fear of Harm behavioral dimension, consists of symptoms that currently reside in numerous diagnostic categories of the DSM-IV. These include parasomnias, obsessive-compulsive and REM sleep behavior disorder, bulimia, anorexia, suicidality and psychosis. FOH sets a new frame around a specific set of highly heritable symptoms and so does not pertain to any specific set of current DSM IV criteria and cannot be diagnosed using accepted nomenclature. How It Was Done: Data Collection The JBRF (Juvenile Bipolar Research Foundation) website has served as a portal for the collection of data on early-onset bipolar disorder. Primarily, information comes in through the submissions of the CBQ. The CBQ was developed to gather a broad range of symptom information about children who were suspect for, or had received a community diagnosis of, a bipolar disorder. The questionnaire asks parents to endorse symptoms from a list of items that, while inclusive of mania and depression, also lists symptoms from a variety of pediatric psychiatric illnesses that are often considered co-morbid with juvenile bipolar disorder (separation anxiety disorder, generalized anxiety disorder, OCD, ODD, CD, and ADHD). Reliable algorithms were developed that could comb through the data and provide preliminarily identification of subjects with 1.) bipolar disorder according to a DSM IV bipolar diagnosis as well as according to various proposed phenotypes, 2.) bipolar disorder with and without comorbid ADHD, and 3.) ADHD with no bipolar disorder. Thus a rapid and flexible scoring system was created that could go through large submissions of data and designate appropriate study groups. Using this screening tool, investigators were able to use over 6,000 profiles for their research. This treasure trove of information continues to grow and provide the robust pools of data needed in order to be able to conduct meaningful analyses. Investigators also collected through the JBRF website, data from YBOCS (the Yale Brown Obsessive Compulsive Scale) and OAS (the Overt Aggression Scale). These well validated screening tools measure anxiety, obsessive-compulsive behaviors and thoughts as well as aggression directed towards self and others. The investigators gathered this information to address the long expressed concern regarding the high incidence of anxiety and aggression amongst these children. The sample size for all studies was in the thousands of subjects. How It Was Done: Studies Investigators made the first important foothold on what would develop into their highly refined subtype of the illness through the use of data from YBOCS and OAS. Examining six items from YBOCS and two items from OAS, they were able to demonstrate a relationship between anxiety and aggression. They found that children with bipolar disorder who were obsessively fearful that harm would come to themselves or others were 2.7 times more likely to inflict serious harm on themselves, and 8 times more likely to inflict serious harm on others, than children from the same group who did not experience obsessive fears. Investigators called this behavioral trait Fear of Harm, or FOH, and the eight items that define it the FOH index. They further found that children characterized by FOH were more likely to threaten suicide than those who werent. This trait was determined not to be found in healthy subjects. Investigators recognized FOH to be not only an alarming behavioral dimension, but also a strong candidate for a defining feature of a unique form of the disorder. (For the full article, click here.)
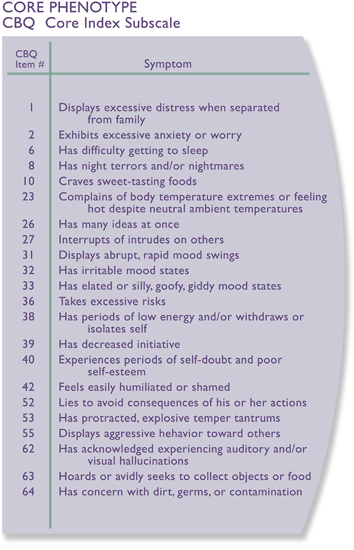
Concurrent to the FOH study, investigators conducted a dimensional analysis on the symptoms endorsed in almost 3,000 CBQs of children at risk for, or who had received a community diagnosis of, bipolar disorder. The study resulted in the clustering of symptoms into ten behavioral dimensions or factors. While the familiar traits of depression and mania were identified, it also clustered a factor which combined symptoms of anxiety and aggression. The appearance of this factor lent support to the FOH relationship from the YBOCS/OAS study. Additionally, the analysis arrived at factors suggestive of behavioral dimensions never before associated with the profile. Amongst those factors are sleep cycle problems, sensory sensitivity and oppositional/poor frustration tolerance; features that many parents of children with bipolar disorder can tell you are inseparable from their daily struggle. Armed with a better dimensional understanding of the illness that these two studies provided, investigators were ready to suggest an alternative phenotype that they felt better defined juvenile bipolar disorder. Central to the criteria were the symptoms of FOH. To this list they added several more CBQ items that demonstrated particular importance during the dimensional analysis. The resulting list of 22 CBQ symptoms is called the Core Phenotype. It is, in their minds, a more accurate list of symptom criteria by which to identify a child at risk for bipolar disorder. (For the full article, click here.) A program on the JBRF website provides scoring of the CBQ that will indicate whether or not a child matches a Core phenotype definition of the illness. (to get to the CBQ and its scoring, click here.)
The next step the investigators took was to determine the heritability of the FOH index, the ten CBQ dimensions and the proposed Core phenotype. Determining heritability is very important as it establishes that the characteristic or symptom under question is inherent to the illness (and thus genetically relevant) rather than brought about through cultural or environmental influences. The results of this inquiry provided investigators with much confidence that they were traveling down a fruitful path. The studies showed that FOH is indeed a highly heritable feature likely rooted in a genetic source. Analysis of the 10 different CBQ factors sorted them into an order of relative heritable importance to the phenotype. The factor that proved to have far and away the greatest concordance, significantly higher than either mania or depression, was the one which linked anxiety or fearfulness with aggression. And the Core phenotype, as a composite of 22 CBQ symptoms, inclusive of FOH, was also found to describe a highly heritable profile. Clearly, investigators were on solid ground to consider FOH as the basis for a genetically identifiable subtype of the disorder. (For the full article, click here.) To learn more about the FOH phenotype investigators hypothesized that as the measure of FOH increased, so too would the severity of selective factors, including mania and depression, and various course of illness factors such as age of onset, hospitalization, school difficulty and involvement with the juvenile justice system. To do this, they first divided a large group of children with a standard diagnosis of bipolar disorder into three groups depending upon their measure of FOH; none, low or high. As it happens, roughly one third of the children fell into each group. Children who fit the highFOH group experienced a significantly greater frequency of manic and depressive symptoms than the other children. Investigators found that the total number of endorsed CBQ items increased significantly as measures of FOH increased. They also determined that, while all three groups experience significant severity of illness measures, the FOH children experience significantly more frequent hospitalizations and increased incidence of school failure.
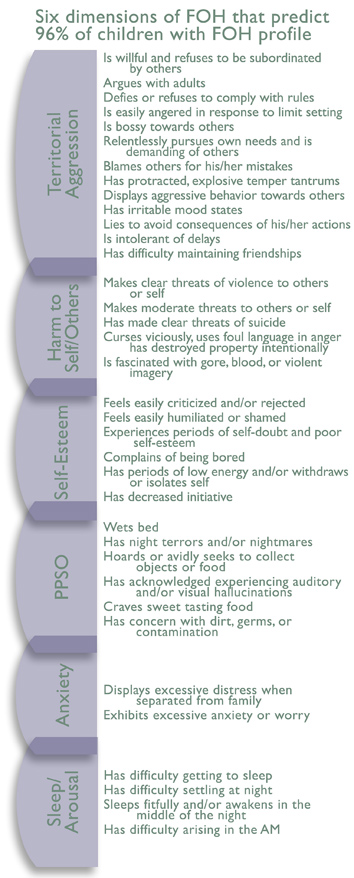
Having established the clinical importance of this subgroup of children, investigators performed another dimensional analysis to determine the symptom-clusters most highly associated with, and predictive of, the FOH trait feature. The new analysis grouped together ten slightly different symptom-clusters than the previous CBQ factor analysis. Taken together, these factors provide a rather complete sense of the experience imposed by this subtype of the illness. The factors were given the dimensional names of territorial aggression, attention/executive function, mania, harm to self/others, self-esteem, sleep, sensory, hypersexuality, PPSO (a combined factor consisting of psychosis, parasomnias, sweet cravings and obsessions/germ contamination fears) and anxiety. Investigators determined that as a childs FOH measure increased, from none to low to high, so too did each one of these factors. But researchers were able to determine that the following six factors; territorial aggression, harm to self/others, self-esteem, PPSO, anxiety and Sleep/Arousal, when taken together, are able to predict 96% of the children who are considered to have the FOH phenotype. (For the full article, click here.) To summarize, the work conducted over the past six years has brought to light a profile of juvenile bipolar disorder that differs substantially from the current conceptualization. The comprehensive set of symptoms brought together in this new phenotype points towards dysregulation of basic homeostatic processes underlying the disorder. Many of the behaviors can be looked at as responses to threats or dysregulation of basic survival systems. To date, the work has defined a highly heritable trait of the disorder that can serve as the basis for examining a more homogeneous subgroup of the illness. That subgroup can be easily identified for both clinical and research purposes and is of great clinical importance as they are the children who are most severely impacted by the illness. The work has also resulted in the identification of a potential biomarker that may provide the basis for confident differential diagnosis. What The New Phenotype Leads ToBreaking through conceptual constraints to develop new ways of thinking about a diagnostic process has been a formidable challenge. Acceptance of this novel view will require an open-mind. JBRF sponsored research is now turning to a genome-wide scan in an effort to track down the genes that cause the susceptibility for the illness. We are optimistic that the delineation of the FOH phenotype will make it more likely that the genome-wide study will be successful. In the meantime, the insights that have resulted from the dimensional study of the disorder have led investigators to develop some clearer ideas of the underlying biology of the disorder. IF YOU WOULD LIKE TO DONATE TO JBRF VIA PAYPAL, PLEASE CLICK HERE. References 1. Cheng, R., Juo, S.H., Loth, J.E., Nee, J., Iossifov, I., Blumenthal, R., Sharpe, L., Kanyas, K., Lerer, B., Lilliston, B., Smith, M., Trautman, K., Gilliam, T.C., Endicott, J., Baron, M., 2006. Genome-wide linkage scan in a large bipolar disorder sample from the National Institute of Mental Health genetics initiative suggests putative loci for bipolar disorder, psychosis, suicide, and panic disorder. Mol. Psychiatry 11, 252260. 2. Mataix-Cols, D., Wooderson, S., Lawrence, N., Brammer, M.J., Speckens, A., Phillips, M.L., 2004. Distinct neural correlates of washing, checking, and hoarding symptom dimensions in obsessivecompulsive disorder. Arch. Gen. Psychiatry 61, 564576. Mataix-Cols, D., Rosario-Campos, M.C., Leckman, J.F., 2005. A multidimensional model of obsessivecompulsive disorder. Am. J. Psychiatry 162, 228238. Mataix-Cols, D., Pertusa, A., Leckman, J.A., 2007. Issues for DSM-V: how should obsessivecompulsive and related disorders be classified? Am. J. Psychiatry 164, 13131314. Mataix-Cols, D.,Nakatani, E.,Micali,N.,Heyman, I., 2008. Structure of obsessive compulsive symptoms in pediatric OCD. J. Am. Acad. Child Adolesc. Psych. 47, 773778. |
|
New: Are you interested in finding out if your children qualify to participate in the JBRF's research studies? Learn more here. Context and Summary of JBRF Sponsored Research Clinical Phenomenological Study of Childhood-onset Bipolar Disorder Neuropsychological Testing in Juvenile-onset Bipolar Disorder |
Top | Home | About JBRF | About Juvenile Bipolar Disorder | Research Studies
Professional ListServs | JBRF Library | In The News | Make A Donation
Our Disclaimer | Privacy Policy | Contact
Web
site designed by flyte new media
email
Web Developer